Article Text

Abstract
Objectives To summarise the rationale, workflow and recommendations for the conduct of exposure assessment critiques in key human studies evaluated for International Agency for Research on Cancer (IARC) Monographs on the Identification of Carcinogenic Hazards.
Methods Approaches to evaluating exposure assessment quality in human cancer and mechanistic studies were reviewed according to the precepts outlined in the IARC Monographs Preamble, using two agents as case studies. Exposure assessment ‘domains’, that is, salient aspects of exposure assessment for the agent under evaluation, were selected for review across the key human studies.
Results The case studies of night shift work (volume 124) and 1,1,1-trichloroethane (volume 130) used a common approach, tailored to the agents’ specific exposure scenarios, to evaluate exposure assessment quality. Based on the experiences of IARC Working Groups to date, the implementation of exposure assessment critique requires the need for agent-specific knowledge, consideration of the validity of time-varying exposure metrics related to duration and intensity, and transparent, concise reviews that prioritise the most important strengths and limitations of exposure assessment methods used in human studies.
Conclusions Exposure assessment has not historically been a fully appreciated component for evaluating the quality of epidemiological studies in cancer hazard identification. Exposure assessment critique in key human cancer and mechanistic studies is now an integral part of IARC Monographs evaluations and its conduct will continue to evolve as new agents are evaluated. The approaches identified here should be considered as a potential framework by others when evaluating the exposure assessment component of epidemiological studies for systematic reviews.
- Epidemiology
- Occupational Health
- Toxicology
- Environmental Exposure
Data availability statement
No data are available.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The quality of exposure assessment methods is a key factor to judge the informativeness of studies involving exposed humans. When reviewing cancer epidemiology studies, exposure misclassification has not always been a main focus when judging study quality and sources of bias. This article describes the efforts in the International Agency for Research on Cancer (IARC) Monographs programme to systematically include a review of exposure assessment quality when evaluating studies of human cancer or mechanisms.
WHAT THIS STUDY ADDS
This study describes in detail how the exposure assessment quality is reviewed during cancer hazard identification performed by the IARC Monographs programme. It shows how using well-defined exposure assessment review domains that are informed by expert knowledge can help to perform consistent and transparent reviews of exposure methods reported in the literature.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A similar approach might be applied by others who review exposure assessment methods, either for systematic reviews, meta-analyses or cancer hazard identification, thereby increasing transparency and consistency in the field.
Introduction
The Monographs Programme of the International Agency for Research on Cancer (IARC) provides a framework for the conduct of expert evaluations to identify carcinogenic hazards to humans that inform public health policies and cancer prevention strategies worldwide. Monographs evaluations entail the synthesis of multiple evidence streams, that is, epidemiological studies of cancer in humans, experimental studies in animals and studies of biological mechanisms of carcinogenesis. The programme’s procedures have evolved in parallel with scientific advances and its Preamble—the document outlining procedures to which evaluations adhere—is revised periodically.1 2 Recognising the importance of exposure assessment in the informativeness of epidemiological studies, recommendations described in the most recent Preamble update included the addition of a critique of exposure assessment methodologies of key studies of cancer in humans and of carcinogen mechanisms in exposed humans.2 Such critiques are integral to judge the informativeness of, and potential for bias in, the epidemiological evidence of cancer and mechanisms synthesised for evaluations. These critiques have since been added to the exposure characterisation section of the Monographs (section 1), which already had served to define agents under evaluation; describe methods for detection and analysis; summarise production, use and occurrence in the environment and consumer products; characterise prevalence and concentrations in human populations and describe regulations and guidelines worldwide.
Since its formalisation in the 2019 Preamble revision, an exposure assessment critique for cancer epidemiology studies has been undertaken for agent evaluations in eight volumes: night shift work (in volume 124), opium (in volume 126), aniline (in volume 127), acrolein and crotonaldehyde (in volume 128), 1,1,1-trichloroethane (in volume 130), cobalt and antimony (in volume 131), occupational exposure as a firefighter (in volume 132), aspartame, methyleugenol and isoeugenol (in volume 134) and perfluorooctanoic acid and perfluorooctanesulfonic acid (in volume 135) and talc and acrylonitrile (in volume 136). Prior to the adoption of the revised Preamble, the exercise had also been undertaken to various extents in earlier evaluations (ie, welding in volume 118, benzene in volume 120 and styrene in volume 121). This article describes and summarises the overarching concepts and approaches used to undertake exposure assessment critiques, presenting two case studies of agents for which these critiques have been employed to date—night shift work and the chemical exposure 1,1,1-trichloroethane.
Methods
Workflow
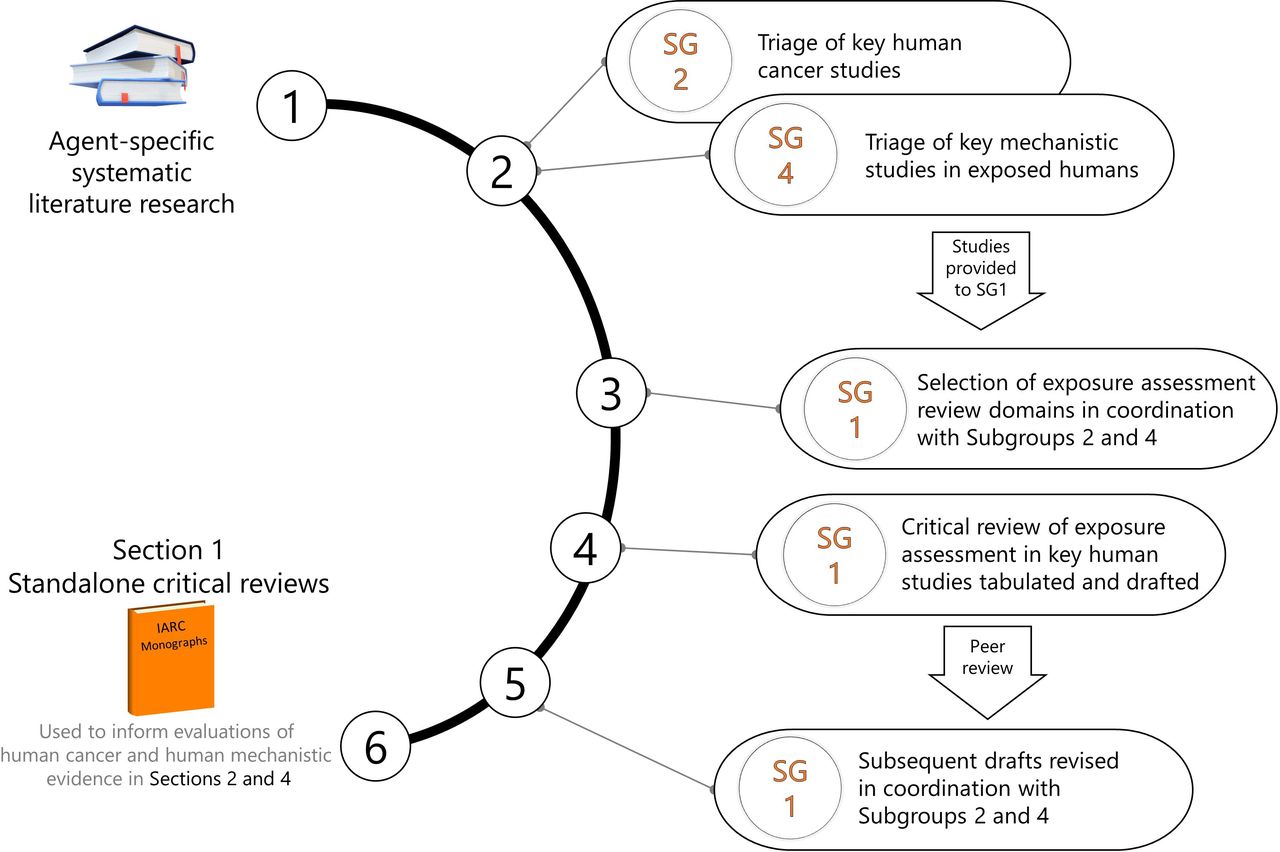
The IARC Monographs evaluation procedure, as described in the latest version of the Preamble,1 involves the critical review and synthesis of evidence by four subgroups of international experts, who characterise human exposure (subgroup 1), and review human cancer evidence (subgroup 2), animal bioassay evidence (subgroup 3), and mechanistic evidence in humans and experimental systems (subgroup 4). The critique of exposure assessment methods in key human studies is the responsibility of subgroup 1 but also involves coordination with subgroups 2 and 4 at various stages of a Monographs evaluation. Key tasks are summarised in the flow diagram in figure 1.

{kind=link}
Flow diagram of a typical workflow of the preparation of an exposure assessment critique for an IARC Monograph. Step 1 is performed by the IARC secretariat and the following steps are carried out by the experts of subgroups 1, 2 and 4 with assistance of the secretariat. IARC, International Agency for Research on Cancer; SG, subgroup.
Identification of key studies
The first task undertaken prior to critiquing exposure assessments is the identification of key human studies. ‘Key studies’ are those deemed to contribute important information to the evaluation’s human cancer and mechanistic evidence streams, from the standpoint of study design and endpoint measurement, but which have not yet been critically evaluated for quality or informativeness of the exposure assessment. Identification of studies is achieved by a triage of identified literature by the subgroups responsible for the evaluation of human cancer studies (subgroup 2) and mechanistic studies in exposed humans (subgroup 4).
Domains of exposure assessment critique
The objective of the IARC Monographs is to identify cancer hazards by assessing the strength of available evidence to indicate that an agent can cause cancer. For the two human evidence streams, this assessment encompasses a judgement of the informativeness (for drawing causal conclusions) of associations between exposure to an agent and either a cancer outcome or a cancer-relevant mechanistic outcome (under the framework of the ‘key characteristics of human carcinogens’3). The quality of the exposure assessment methods employed in key studies is thus one of the most important factors to judge the informativeness of an association. Put simply, ‘quality’ in this context refers to the likelihood that the exposure assessment reflects the study population’s true exposure to the agent of interest with a minimum of mismeasurement or misclassification, and whether this likelihood is sufficient to demonstrate a true association. The assessment should also reflect the variation in exposure both within the study population and over time. Thereafter, conclusions about the quality of exposure assessment are also used by subgroups 2 and 4 to judge the potential for exposure measurement error or exposure misclassification that may lead to bias in the estimates of association between the agent and outcomes of interest, namely cancer or mechanistic endpoints.4 The quality of assessment of coexposures may also be important as the coexposures can result in confounding if they are both associated with the agent being evaluated and also cause the cancers (or mechanistic endpoint) of interest.
The scope of exposure assessment review differs from one agent to another due to the unique characteristics of the agents under review and different study designs and specific measurement methods. However, a common framework has been established and is outlined here. The first task of subgroup 1 is to propose and agree on a set of ‘domains’ for the critique of methods used for a given agent. These domains are considered the salient aspects of exposure assessment that affect the informativeness of the epidemiological studies reviewed. The Monographs require a specific description and appraisal of these domains. Examples of domains common to many agents are exposure definition (how did the study define exposure to the agent?); duration (what information was available on the amount of time participants were exposed?) and intensity (how was intensity estimated and, if the exposure changed over time, was the level of exposure quantified at given points in time?). Other domains are more specific to given agents, such as the route of exposure; the definition of exposure groups; and the assessment of coexposures that may potentially confound associations (eg, for chemicals used in industrial settings where simultaneous exposure to other potentially carcinogenic agents may occur). Ideally, information on sensitivity and specificity of the exposure assessment is available to permit the consideration of the potential for bias from exposure measurement error and misclassification. The potential for recall bias to cause differential exposure misclassification is also considered.
After initial identification of the key human studies by subgroups 2 and 4, subgroup 1 identifies important exposure domains and tabulates them to aid the human study review process. Each study is then reviewed by subgroup 1, and a description of how the study considered each domain is developed. While the domains are rooted in exposure science and epidemiological concepts applicable to multiple agents, they are tailored to the specifics of each agent of interest as informed by a thorough scientific review of assessments of exposure. For most volumes, the exposure experts of subgroup 1 reach a consensus on these domains based on the available literature and their expertise. For example, in the evaluation of night shift work, published recommendations from a previous workshop convened by IARC were instrumental in identifying relevant domains for this agent.5 A subsequent workshop addressed research gaps and recommendations for a wider group of agents with unresolved carcinogenicity, highlighting the importance of exposure assessment quality in evidence evaluations.6 7
Lastly, a summary appraisal of the strengths, limitations and potential for inducing bias (and its potential direction) in the exposure-and-outcome relation is made. This framework allows subgroup 1 members to focus on the most important aspects of the methodology and formulate a summary and overall critique for each study, which is provided to subgroups 2 and 4 for their review as they evaluate the studies. Exposure assessment questions that may arise during review by subgroups 2 and 4 are then communicated with subgroup 1. The questions may quickly be answered, or a meeting of the subgroups may be required to reach consensus on the structure and content of the exposure assessment critiques. Ultimately, the critique is used to interpret the informativeness of the studies and the potential for and, if possible, degree and direction of, bias arising from the exposure assessment methods and from confounding in key human studies with respect to evaluation of risk of cancer (or mechanistic endpoint) following exposure to the agent of interest. Subgroup 1 then finalises the critical reviews in chapter 1 and reviews the evaluations by subgroups 2 and 4 to ensure the weight they place on the assessment and interpretation regarding informativeness and the potential of bias is consistent with subgroup 1’s assessment.
Tables 1 and 2 show the domains used for the critical appraisal of exposure assessments in key studies of night shift work and 1,1,1-trichloroethane, respectively, which are discussed below.
Excerpts of representative studies to illustrate how some of the domains were tabulated for the critical appraisal of exposure assessments in key studies of night shift work (NSW)
Excerpts of representative studies to illustrate how some of the domains were tabulated for the critical appraisal of exposure assessments in key studies of 1,1,1-trichloroethane
Night shift work
Night shift work, evaluated by the IARC Monographs Volume 124 Working Group,8 was the first Monographs evaluation undertaken after the formal addition of exposure assessment critical reviews as part of the revised Preamble.2 Key human cancer studies were numerous, with epidemiological investigations employing different designs (cohort, nested case–control, case–control). Study populations included night shift workers in healthcare and industrial settings, as well as those in the aviation industry flying through multiple time zones. A workshop convened by IARC and described in Stevens et al 5 was instrumental in assisting the Working Group’s development of domains of exposure assessment for examination in the volume 124 evaluation (table 1).5 Studies were assessed for their definition of night shift work and categorised as follows: (1) defined, including ≥3 hours of work between 23:00 and 06:00 hours or a flight of ≥3 hours between 22:00 and 08:00 hours (local departure time); (2) defined, other or (3) undefined. The first operational definition reflected exposure to work during the biological night (typically including the time frame from 23:00 to 7:00 hours am that most adults use for sleeping); studies using this definition were considered of higher quality for this reason (further, this definition allowed for cross-study comparisons), whereas findings from studies under the third category (undefined exposure) were considered of lower quality because the exposure groups may have included participants with drastically different exposures, including those not working during the biological night. Two domains assessed efforts made by study investigators to quantify night shift work exposure. These were intensity of exposure to night shift work—the number of night shifts performed within a certain time period; and duration of exposure to night shift work—years spent undertaking night shift work. The subgroup assessed studies for the precision and completeness of these two domains, respectively. Other domains were considered. For example, the type of assessment domain assessed how information on night shift work was collected in each study: objective (eg, work rotas), subjective (eg, interview data) and job-exposure matrix (JEM) assessments.
As exposure misclassification in the reference group (eg, the reference group is considered to be unexposed but includes exposed participants) is an important consideration in research focused on night shift work, this domain was included for assessment—‘reference group: past or present schedule includes night shift work’. For studies included in the ‘yes’ category of this domain, the absence of possibly exposed study participants in the referent group could not be verified. The main concern with this domain (which has been generalised in many subsequent evaluations of agents in the Monographs programme) was a downward bias in estimates of the association between night shift work and cancer. Additional domains with lesser bearing on the informativeness of studies, though of possible utility to explaining study heterogeneity, were temporality of exposure to night shift work—start and end dates of night shift work; type of night shift work schedule—for example, differences between permanent and rotating schedules; number of consecutive night shifts; direction of night shift rotation—the ordering of subsequent shifts (eg, clockwise vs counter-clockwise rotation); and start and end times of all shifts, which provides additional information on exposure to night work during the biological night.
One concern common to many of the cohort studies reviewed was a lack of information on night shift work at points in time after the baseline questionnaire, which was noted to have likely resulted in risk estimates that were biased towards the null. A major concern noted for case–control studies, which tended to have more detailed information on exposure to night shift work, was possible recall bias among cases compared with controls. The Working Group noted, however, that there was little empirical information to support the assessment of such biases in night shift workers. These exposure quality considerations were central to the conclusion that there was limited evidence for the carcinogenicity of night shift work for cancers of the breast, prostate and colorectum in humans.
Chemical exposure: 1,1,1-trichloroethane
Several chemical exposures have been evaluated by the IARC Monographs programme. The domains for the critique of their exposure assessment methods took a different form from those compiled for night shift work. The evaluation of aniline (volume 1279) has served as a template that has been adapted for subsequent evaluations dealing with chemical exposures, including in volumes 128, 130 and 131.10–12
1,1,1-Trichloroethane was evaluated by the IARC Monographs Working Group in Volume 130 and will be discussed as an example of a chemical exposure.11 Key human cancer studies investigating 1,1,1-trichloroethane exposure consisted of two cohort studies (of Finnish workers exposed to halogenated hydrocarbons and of aircraft maintenance workers in the USA), 5 nested case–control studies, 16 population-based case–control studies and 3 case reports. The domains for the critique of 1,1,1-trichloroethane exposure assessment methods (table 2) were adapted from the template established by the volume 127 aniline evaluation and consisted of the exposure definition; whether the assessment was qualitative, semiquantitative or quantitative and the assessment of exposure intensity (from measurement data or estimated from job and task), duration (from employer records or self-reports) and cumulative exposure (derived from intensity and duration). Other domains were exposure assessment methods (including data source, environmental and biological measurements); appropriateness of sampling and collection protocols for environmental or biological measurements (ie, whether the protocols followed accepted methods); route of exposure assessed (inhalation and dermal); timing of exposure relative to outcome; other carcinogenic exposures (based on the study information or on knowledge of the jobs and industries) and misclassification of unexposed (referent) group (how the group was characterised).
The exposure assessment critique undertaken by subgroup 1 for this agent found that it was often difficult to confirm the presence of 1,1,1-trichloroethane, particularly in population-based case–control studies due to its use in product mixtures and its varying interchangeability with other chlorinated solvents over time. Concerns regarding mixtures and interchangeability originated from information external to the key studies, resulting in the potential for exposure misclassification or possible confounding. Other important considerations were the lack of detailed job histories and few exposure measurements for some studies, and the inability to differentiate workers based on exposure intensity, duration, or probability. Most of these issues were thought to result in attenuation of exposure-response associations. The use of grouped data in establishing JEMs was thought to lead to loss of statistical precision, but not bias, in exposure-response estimates. In summary, the evaluation of exposure assessment quality was instrumental in reaching the evaluation of limited evidence in humans for the carcinogenicity of 1,1,1-trichloroethane, with credible associations observed for multiple myeloma.
The aforementioned examples focus mainly on the review of exposure assessment domains for the human cancer studies, since the formal approach was first implemented for section 2 on human cancer studies. In addition, during the evaluation of night shift work (volume 124), some domains developed by subgroup 1 for human cancer studies were also used to assess the informativeness of mechanistic studies by subgroup 4, even though this volume did not include a standalone section on this information. For volume 130, subgroup 1 applied the same domains to review the exposure assessment of 1,1,1-trichloroethane in both human cancer and mechanistic studies in humans. Critiques included the potential for coexposure in one mechanistic study which influenced subgroup 4’s judgement of the study’s informativeness.
For subsequent evaluations of chemical agents, the set of domains used for chemical agents continues to be refined and expanded as appropriate for the agent under evaluation. There are some domains such as the agent definition, the exposure assessment methods used and the potential for misclassification that have been commonly used, whereas some other domains were more agent-, and therefore, volume-specific (see table 3). Human cancer studies evaluated in the IARC Monographs are generally either cohort or case–control studies. Mechanistic studies involving exposed humans have displayed a larger diversity of study designs, including cross-sectional studies, cohort studies, intervention studies, randomised control trials and case series and might include short-term and long-term exposures. To account for this, the information on exposure assessment for the mechanistic studies can be more diverse between studies or agents and focus more on specific aspects. For example, working groups have paid specific attention to the timing of exposure assessment respective to the dynamics of the biological endpoints under study.
Examples of exposure assessment review domains that have been used in most critical exposure assessment reviews since volume 124 and those that have been used in only one or few reviews
Discussion
Formal exposure assessment critiques are a relatively recent addition to IARC Monographs evaluations, and therefore, continue to evolve in their approach. Their ultimate conduct and form depend on several factors, including the nuances of specific agents under evaluation, the information provided in the key studies, and the knowledge-based judgement of subgroup experts. The choice of exposure assessment domains is made by experts for the given agent; therefore, the critiques are likely to reflect the most important study characteristics needed to judge their quality. The process includes a systematic review of the exposure assessment of all key studies, which increases consistency within and across the Monographs. Describing the strengths and limitations of each study increases the transparency of the decisions made by the Working Groups. Sources of bias, and where possible, the direction and amount, are made explicit.
The following points are based on the experience of conducting exposure assessment critiques since their introduction to Monographs procedures. They highlight overarching scientific and practical considerations underpinning efficient and informative critiques of exposure assessment performed in key human studies during the Monographs evaluation:
To make the process as efficient as possible, emphasis should be on the most important aspects of the exposure assessment. For example, if a study is severely limited because exposure measurement occurred well after cancer treatment, or because exposure to the agent could not be separated from other carcinogenic coexposure(s), minor details of analytical protocols are of less importance and do not need to be acknowledged in detail.
Similarly, exposure assessment critiques should focus only on aspects of exposure assessment (subgroup 1) while other aspects of the design, outcome ascertainment, statistical analysis, assessment of other biases and results interpretation are the responsibility of subgroups 2 and 4. That is not to say that information under the purview of another subgroup cannot be considered in the exposure assessment review. For example, the knowledge of the type of study design (cohort or case–control) may impact the evaluation of the presence of the agent (there may be greater certainty of exposure in cohort studies of particular industries than in population-based case–control studies).
Regular communication between subgroup members throughout the review process greatly increases the utility and efficiency of critiques and ensures that there is consistency in the interpretation of the quality of the exposure assessment. It also aids knowledge transfer from experts in subgroup 1 with expertise in analytical chemistry and exposure assessment to the epidemiologists and toxicologists of other subgroups and brings to the fore concerns regarding exposure assessment quality in the final evaluation. Critical information about absorption, distribution, metabolism and excretion, which is typically evaluated in subgroup 4, may inform the evaluation of exposure assessment quality by subgroup 1, such as the timing of a biological measurement relative to exposure.
Exposure assessment critiques for mechanistic studies in exposed humans have been introduced more recently, and therefore, there is less experience with this process. The design and diversity of mechanistic studies tend to differ from human cancer studies, which can make the review of exposure assessment more challenging. Previous evaluations have shown, however, that similar exposure assessment review domains can often be applied to both mechanistic and human cancer studies.
A more general observation, also applicable in contexts outside of the Monographs programme, is that an in-depth understanding of the exposure science specific to the agent under review is essential to the development of appropriate domains for the critique of exposure assessment methods, which might need to be very agent-specific.13 This was exemplified in the case study of night shift work, in which the importance of the exposure definition was recognised and applied in the critique. Knowledge obtained from studies external to the key studies also was important in identifying possible coexposures, particularly in case–control studies, where exposure to 1,1,1-trichloroethane was considered possible but was not definite due to the interchangeability of many chlorinated solvents. Clearly defined exposure assessment quality domains are crucial for any objective, transparent and consistent review of studies in exposed humans. Past examples from recent Monographs evaluations show that there are common domains that are needed to judge the quality of exposure assessment for most agents (table 3).
Other approaches to examine exposure assessment in observational epidemiology studies include algorithmic tools such as the ‘Risk of Bias in Non-randomised Studies-of Environmental Exposure’.14 Such tools emphasise the potential for bias as determined systematically by reviewers, rather than the Monographs’ expert-based appraisal of the quality and informativeness of the exposure data for addressing the causal question about exposure to an agent and cancer. Furthermore, these algorithmic tools do not have a very detailed focus on the exposure assessment necessitating a separate approach to judge the quality of the exposure assessment in human observational studies.13 Our approach lends itself well to examining the impacts of potential biases resulting from the exposure assessment approach taken and judging which studies are likely to provide the most informative results on the basis of exposure assessment quality.4
In conclusion, critiques of exposure assessment in key human studies are now an integral part of IARC Monographs evaluations, which has greatly aided Working Groups to assess the informativeness of evidence under evaluation. The approaches summarised in this article will continue to evolve as a wider variety of different agents are evaluated. A focus on exposure assessment is becoming more important in systematic reviews,4 and we recommend that guidelines for systematic reviews should include a formal assessment of the quality of exposure assessment and its impact on causal inference.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not required.
Acknowledgments
We thank Solene Quennehen for her assistance with the creation of the figure. The contributions of all Working Group members, IARC Secretariat and technical staff for meetings 124 and 130 are gratefully acknowledged.
References
Footnotes
DRSM and RW contributed equally.
Contributors Study conception and design: DRSM, RW, MKS-B; draft manuscript preparation: DRSM and RW; responsible for the overall content as guarantor: MKS-B; all authors discussed the results and commented on the manuscript.
Funding The IARC Monographs programme receives funding from the National Cancer Institute and the National Institute of Environmental Health Sciences (5R01CA033193-40) and the European Commission Directorate General for Employment, Social Affairs and Inclusion.
Disclaimer Where authors are identified as personnel of the International Agency for Research on Cancer/WHO, or of the Government of Canada, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/WHO or of the Government of Canada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.